I decided to do an update as I get occasional e mails from people who found my blog asking how I am now.
Four years ago I went back on the standard dose of 50mg Sertraline (Zoloft if you're in America) and fairly rapidly made a full recovery. Some months later I got fed up of the "feeling a bit too happy/high even in inappropriate circumstances thing", or the "totally numb" thing (if you're taking these pills you'll know what I mean, if you're not taking these pills you might think it all sounds rather nice).
So long story short, I went back to liquid Prozac and reduced down to 3ml liquid Prozac, every day for the past 2/3 years I have been taking exactly 3ml liquid Prozac (standard dose is 5ml). This particular dose means I ditch the numbness, but I haven't reduced so much that I go into acute withdrawal/depression/anxiety/dread mode. It works perfectly for me and I'm leading a "normal" life, whatever "normal" is, and I don't often think about it unless someone asks.
Yes depression/anxiety always lurks beneath the surface, you never really get rid of it. Sometimes something will trigger an attack of insomnia/anxiety, or a wave of depression, but I can generally get a grip on it or ride it out.
Thursday, 6 July 2017
Friday, 19 July 2013
One journey ends and another one begins
This is my last blog post it’s time for me to move on. My page on Facebook will also be deleted shortly.
I tried, I gave it my best shot, it didn’t work out, and
if I hadn’t tried I’d never know and
I’d still be wondering.

Reader, I went to the doctor and I started the
Sertraline. I read somewhere “being mentally ill sucks, the drugs suck, it’s
choosing the least sucky option”. The decision was not made lightly, but having
made the decision I felt like a great weight had lifted off me, devastated and
totally drained, I was off work for 2 weeks, I needed that space to come to
terms with my decision and what had happened.

Whether I like it or not, I have been feeling a lot better. I’m
relieved to be feeling better, and trying not to think too hard about whether
there are any long term implications to being dependent on a drug, and take one
day at a time.
This decision is the right one for me at this point in time, it wasn't all bad, the tapering method worked for me for a long time and it works for many other people who have successful outcomes, who knows, I might revisit it at some time in the future.
I discovered the meaning of my recurring dream.
Something positive to have come out of this journey is that I’ve discovered I have some absolutely fantastic supportive friends in real life and on line, and a fantastically supportive husband and parents.

In the middle of June 2013 I’d had enough, had enough of overwhelming
depression that wasn’t going anywhere, and the persistent feelings of dread and
anxiety. I couldn’t cope with the fact that I couldn’t cope with doing routine
things like going to work and participating in normal everyday things. This may
have been withdrawal, but this was also very real depression. There were odd
good days but I began to realise that I was kidding myself, I wasn’t getting
any better, I was trying hard, lots of bike rides, healthy diet, positive
thinking. It came to a head when I couldn’t get myself into work one morning,
and I just couldn’t fight it anymore, I felt crippled by it. I’d been debating
for a few weeks whether to go back to Sertraline.

This decision is the right one for me at this point in time, it wasn't all bad, the tapering method worked for me for a long time and it works for many other people who have successful outcomes, who knows, I might revisit it at some time in the future.
Something positive to have come out of this journey is that I’ve discovered I have some absolutely fantastic supportive friends in real life and on line, and a fantastically supportive husband and parents.
Wednesday, 29 May 2013
It's Getting Better all the Time (kind of)

If you'd asked me, this time last year, I would've said I was doing really well, and well on course to be off Prozac completely in the near future. I was even thinking this blog would be all tied up and finished and left just floating around in cyber space.
At one point though, I was feeling so bad I was considering going back to the full dose and being done with it, the thing that stopped me was the thought of the horrible side effects, the numbing of libido and emotions, and there is a tendency to essential tremor in my family and I notice on the drug, full dose, my hands have a horrible tremor, and my handwriting gets really scruffy, and I'm enjoying my piano, so no I don't want to aggravate a tendency to a tremor which the full dose gives me.
P and I have talked over this so much, we've come to the following conclusions:
- I have an underlying condition/predisposition to depression/anxiety.
- The drug is too enmeshed in my brain/body after so many years which have included various attempts at cold turkey and alternate day withdrawals messing up my nervous system.
I genuinely feel that it's been too many years now, and I can't put myself through the misery of withdrawal any more, I'm sooo tired of it, it's not what I thought would happen but I'm going to stay at 8mg, possibly forever, I'm at a point where I want to keep quality of life, and after you've been through a period of depression and come out the other side, boy does life feel good, I think you never take "happiness" for granted if you've experienced depression.
I'd like to have got off Prozac fully, but it's not fair on me or my family to keep putting myself through the misery, and since I would probably have to go into "rehab" for a couple of years to do it which isn't an option on the NHS or living in the real world, I can't see it happening. As long as my surgery doesn't have an issue with prescribing the liquid so I can continue with 8mg.
Monday, 6 May 2013
Friday, 5 April 2013
2ml (8mg)
Another up dose :(
Good days and bad days, I think the good days are way out numbering the bad days now, but the bad days feel....bad.
I've tried throwing everything at it, mindfulness, relaxation CD's, my piano, positive affirmations, magnesium, nope, none of this truly shifts a full blown anxiety attack in full flow. Lately, on a bad day, I've caught myself thinking about going back to full dose. Then on a good day I wonder what I was thinking, having got so far.
Good days and bad days, I think the good days are way out numbering the bad days now, but the bad days feel....bad.
I've tried throwing everything at it, mindfulness, relaxation CD's, my piano, positive affirmations, magnesium, nope, none of this truly shifts a full blown anxiety attack in full flow. Lately, on a bad day, I've caught myself thinking about going back to full dose. Then on a good day I wonder what I was thinking, having got so far.
Friday, 22 March 2013
1.30ml (5mg) - Remember that Light at the end of the Tunnel?
Well I think in the end it was an oncoming freight train.
I never really seemed to get any better, many insomniac nights and anxious
low level depressed days, so hard to keep functioning and so very exhausting.
It’s in my nature to soldier on regardless, I’ve always been Mrs Reliable,
always turn up when I say I’m going to turn up, never off sick, whole years
with no sick leave, always do what I say I’m going to do. Now I feel like Mrs Flaky
and unreliable. I never know from one day to the next how I’m going to be. I
must be a great actress though, no one seems to believe me and everyone tells
me I always seem the same and I hide it well. Either I should be on the stage or they’re
being polite I can’t work out which.
P has been trying to persuade me for ages to go for another up dose, so since nothing else seems to be working, and I’m desperate to feel better, we settled on 1.30ml (5mg), this could either go well, or totally backfire, anyone who knows anything about drug withdrawal or reinstatement knows that recovery comes in "waves" and "windows" and as I've had a lot of lovley "windows" this week I'll choose to be optimistic that the "windows" of getting better will increase and the "waves" will decrease.
 I’m one week into the up dose and it’s been a bit of a
roller coaster week, initially I felt like a plant that’s been starved of water
coming back to life, all the anxiety and dread cleared, as though someone had
waved a magic wand, I felt so well the contrast made me realise just how “unwell”
I’ve really been feeling the past 6 months. On day 3 in the evening I had
intense anxiety and dread kick in, had a poor night and woke to very very
intense anxiety, it can be so intense and physical it can reduce me to tears. I was working with P that day and decided to
soldier on, as the day wore on the intense anxiety lifted again and I was well
again. The next day at my other job was all good, I felt great, the following
day was ok and then last night moderate anxiety kicked in again and I was wired
and awake all night. I need to give it a few weeks and see if I settle
down. In any case I’ve almost come to the conclusion that I might never achieve
my goal of all the way off the drug without being so ill that my whole life
goes down the pan, and I might just have to find a permanent stable dose and
stick with it.
I’m one week into the up dose and it’s been a bit of a
roller coaster week, initially I felt like a plant that’s been starved of water
coming back to life, all the anxiety and dread cleared, as though someone had
waved a magic wand, I felt so well the contrast made me realise just how “unwell”
I’ve really been feeling the past 6 months. On day 3 in the evening I had
intense anxiety and dread kick in, had a poor night and woke to very very
intense anxiety, it can be so intense and physical it can reduce me to tears. I was working with P that day and decided to
soldier on, as the day wore on the intense anxiety lifted again and I was well
again. The next day at my other job was all good, I felt great, the following
day was ok and then last night moderate anxiety kicked in again and I was wired
and awake all night. I need to give it a few weeks and see if I settle
down. In any case I’ve almost come to the conclusion that I might never achieve
my goal of all the way off the drug without being so ill that my whole life
goes down the pan, and I might just have to find a permanent stable dose and
stick with it.
In other news I have my new piano at last, electric so I can practise with headphones and not disturb anyone; this is a great way of just getting lost in the moment and so relaxing.
At this point here, I want to say thank you to my husband, my parents and a couple of friends in real life who’ve been so supportive and been there for me going through this, I think they’ll know who they are if and when they read this.
P has been trying to persuade me for ages to go for another up dose, so since nothing else seems to be working, and I’m desperate to feel better, we settled on 1.30ml (5mg), this could either go well, or totally backfire, anyone who knows anything about drug withdrawal or reinstatement knows that recovery comes in "waves" and "windows" and as I've had a lot of lovley "windows" this week I'll choose to be optimistic that the "windows" of getting better will increase and the "waves" will decrease.
 I’m one week into the up dose and it’s been a bit of a
roller coaster week, initially I felt like a plant that’s been starved of water
coming back to life, all the anxiety and dread cleared, as though someone had
waved a magic wand, I felt so well the contrast made me realise just how “unwell”
I’ve really been feeling the past 6 months. On day 3 in the evening I had
intense anxiety and dread kick in, had a poor night and woke to very very
intense anxiety, it can be so intense and physical it can reduce me to tears. I was working with P that day and decided to
soldier on, as the day wore on the intense anxiety lifted again and I was well
again. The next day at my other job was all good, I felt great, the following
day was ok and then last night moderate anxiety kicked in again and I was wired
and awake all night. I need to give it a few weeks and see if I settle
down. In any case I’ve almost come to the conclusion that I might never achieve
my goal of all the way off the drug without being so ill that my whole life
goes down the pan, and I might just have to find a permanent stable dose and
stick with it.
I’m one week into the up dose and it’s been a bit of a
roller coaster week, initially I felt like a plant that’s been starved of water
coming back to life, all the anxiety and dread cleared, as though someone had
waved a magic wand, I felt so well the contrast made me realise just how “unwell”
I’ve really been feeling the past 6 months. On day 3 in the evening I had
intense anxiety and dread kick in, had a poor night and woke to very very
intense anxiety, it can be so intense and physical it can reduce me to tears. I was working with P that day and decided to
soldier on, as the day wore on the intense anxiety lifted again and I was well
again. The next day at my other job was all good, I felt great, the following
day was ok and then last night moderate anxiety kicked in again and I was wired
and awake all night. I need to give it a few weeks and see if I settle
down. In any case I’ve almost come to the conclusion that I might never achieve
my goal of all the way off the drug without being so ill that my whole life
goes down the pan, and I might just have to find a permanent stable dose and
stick with it. In other news I have my new piano at last, electric so I can practise with headphones and not disturb anyone; this is a great way of just getting lost in the moment and so relaxing.
At this point here, I want to say thank you to my husband, my parents and a couple of friends in real life who’ve been so supportive and been there for me going through this, I think they’ll know who they are if and when they read this.

Thursday, 28 February 2013
5th Anniversary of my Blog
Yup I can't believe it's 5 years since I started this, privately, and I thought I would be finished by now and this blog would be all neatly tied up and finished, but no I'm still here with a Facebook page to boot, and a job in addition at: Surviving Antidepressants.
ONE day this will be history.

My Prozac Reduction Timeline
ONE day this will be history.

My Prozac Reduction Timeline
Thursday, 17 January 2013
There IS light at the end of the tunnel - and no I don't think it's an oncoming freight train.
My younger son who takes an interest in this blog came up with the heading for this blog post, and his sense of humour is a bit of a worry.
 Oct/Nov/Dec saw me unravelling in a nightmare way, the
worst things were the fairly severe internal anxiety and adrenaline surges, and
resultant insomnia, I’m a bit scared to publish this but in the interests of an
honest log of my progress here goes, at my lowest points, a few nights saw me
self medicating with tamezapam and whisky, either one, or the other or both
together, 2 or 3 hours of total oblivion even with a hangover the next day was slightly better than 7/8 hours of
sleepless anxiety with someone snoring beside me, only slightly better and it was the bit of
oblivion I was after. The tamezapam has virtually all gone now and I won't get anymore and I've abandoned the whisky, especially after reading alcohol is no good for damaged nervous systems anyway.
Oct/Nov/Dec saw me unravelling in a nightmare way, the
worst things were the fairly severe internal anxiety and adrenaline surges, and
resultant insomnia, I’m a bit scared to publish this but in the interests of an
honest log of my progress here goes, at my lowest points, a few nights saw me
self medicating with tamezapam and whisky, either one, or the other or both
together, 2 or 3 hours of total oblivion even with a hangover the next day was slightly better than 7/8 hours of
sleepless anxiety with someone snoring beside me, only slightly better and it was the bit of
oblivion I was after. The tamezapam has virtually all gone now and I won't get anymore and I've abandoned the whisky, especially after reading alcohol is no good for damaged nervous systems anyway.
I also had a lightbulb moment about a multivitamin I was taking, I'd read that too many B vitamins can be aggravating to messed up nervous systems so I looked at my Holland and Barret vitamin bottle (other brands are available) and discovered that I was taking over 100% of the RDA, so I ditched them and just sticking with the high EPA fish oil capsules and a healthy diet.
Mid December I realised I’d got to guesstimate the best dose of Prozac and stick to it for better or worse, messing about with the dose was sending my nervous system into constant turmoil. Just before Christmas I could feel myself starting to come out the other side, somewhat, the internal anxiety, dread and adrenaline surges subsided, but knew I still had a little way to go to get stable again. There was a fair bit of “faking it to make it” through December, in other words I had to get a grip and force myself through the motions of whatever I had to do on any given day, whether it was work, working with P or Christmassy preparations, but "going through the motions" is grim.
Now into January, I can feel myself feeling more like my old self again, my normal sleep pattern is coming back, not 100%, still getting odd bad nights but definite improvements and feeling more normal, whatever that is, "normal is a setting on a washing machine" comes to mind.
Oct/Nov/Dec saw me unravelling in a nightmare way, the
worst things were the fairly severe internal anxiety and adrenaline surges, and
resultant insomnia, I’m a bit scared to publish this but in the interests of an
honest log of my progress here goes, at my lowest points, a few nights saw me
self medicating with tamezapam and whisky, either one, or the other or both
together, 2 or 3 hours of total oblivion even with a hangover the next day was slightly better than 7/8 hours of
sleepless anxiety with someone snoring beside me, only slightly better and it was the bit of
oblivion I was after. The tamezapam has virtually all gone now and I won't get anymore and I've abandoned the whisky, especially after reading alcohol is no good for damaged nervous systems anyway.I also had a lightbulb moment about a multivitamin I was taking, I'd read that too many B vitamins can be aggravating to messed up nervous systems so I looked at my Holland and Barret vitamin bottle (other brands are available) and discovered that I was taking over 100% of the RDA, so I ditched them and just sticking with the high EPA fish oil capsules and a healthy diet.
Mid December I realised I’d got to guesstimate the best dose of Prozac and stick to it for better or worse, messing about with the dose was sending my nervous system into constant turmoil. Just before Christmas I could feel myself starting to come out the other side, somewhat, the internal anxiety, dread and adrenaline surges subsided, but knew I still had a little way to go to get stable again. There was a fair bit of “faking it to make it” through December, in other words I had to get a grip and force myself through the motions of whatever I had to do on any given day, whether it was work, working with P or Christmassy preparations, but "going through the motions" is grim.
Now into January, I can feel myself feeling more like my old self again, my normal sleep pattern is coming back, not 100%, still getting odd bad nights but definite improvements and feeling more normal, whatever that is, "normal is a setting on a washing machine" comes to mind.
At the moment, I just want to relish feeling “normal” for
a few or even many months, I am torn between feeling desperate to get off this last 1ml of medicine
drug poison, and terrified to rock the boat and do anything about it.... ever.
As an aside, a colleague at work asked me the other week, is there no help or withdrawal specialists on the NHS? really?!?! Yes really!!
I am grateful to P for being my rock, and to Alto Strata and other friends at Surviving Antidepressants, and my nurse friend, for helping me untangle this and work out the best dose to be on.
As an aside, a colleague at work asked me the other week, is there no help or withdrawal specialists on the NHS? really?!?! Yes really!!
I am grateful to P for being my rock, and to Alto Strata and other friends at Surviving Antidepressants, and my nurse friend, for helping me untangle this and work out the best dose to be on.
Monday, 24 December 2012

Sunday, 16 December 2012
A Little Knowledge Can Be a Dangerous Thing!
Yesterday, my friend who is a specialist nurse called round and we talked syringes. (I really need to get a life). This friend is the only health professional me and P know who has taken on board and taken an interest in my issues. I happened to mention in the course of the conversation that I'd started flushing the syringe in water and drinking the water to make sure I got all the medicine out. I'd read that this was a good idea. She pointed out to me that if I had just started doing this, I had inadvertently been updosing another .05ml so I had gone up from 0.85ml to most likely 1.10ml which was a bigger jump than I had intended. I was flusing the Prozac out of the nub at the bottom and that nub is quite big.
 |
| 1ml Syringe |
Everyone close to me has had a different opinion on what I should do, but I decided to go with my gut feeling and go to 1ml. Six days later I think this gut feeling is begining to pay off, this week end the awful gut churning anxiety/dread/doom feelings seem to have just melted away, I'm sleeping better, not quite as well as previously but noticably better and today I feel a definate shift towards feeling more "normal" self again. I have also been practising a mindfulness meditation everyday and of course that may have helped as well.
Saturday, 15 December 2012
1ml (4mg) - Who Needs Red Bull!
So after nearly a month at 1.05ml I honestly wasn’t feeling
any improvement, in fact I think I was beginning to feel worse again, the main
problem was feeling “wired” or like I’d drunk a jug of Red Bull and unable to
sleep, this in turn was making me feel really depressed.
I would really like to thank Alto Strata at http://survivingantidepressants.org/ who asked a knowledgeable doctor about what was happening to me and the conclusion was that by going to 1.05ml I may have overshot my bolt, and the Prozac was becoming too activating, it is a stimulating drug and I seem to be very sensitive. When we studied it I was beginning to feel better shortly after I went to 1.05ml but since Prozac takes a lot of days to reach “high tide” it was probably the effect of going up to 1ml beginning to take effect and then I ramped it up by going up further to 1.05ml and got worse again. So I’m going to see how back to 1ml goes.
In my real life I seem to be surrounded by people who just “stopped” their drug or had no problems, I am so thankful for the internet and finding that I’m so NOT alone with this and I'm not mad.
 In the meantime I have begun to practise mindfulness, and
can thoroughly recommend a book called “The Mindful Way Through Depression”, it
has a CD with it and I’ve begun to do about half an hour practise a day, and if
I can find the right dose to get my nervous system back on the right track I’ll
stick there because I’ve had enough of this crap for now.
In the meantime I have begun to practise mindfulness, and
can thoroughly recommend a book called “The Mindful Way Through Depression”, it
has a CD with it and I’ve begun to do about half an hour practise a day, and if
I can find the right dose to get my nervous system back on the right track I’ll
stick there because I’ve had enough of this crap for now.
My Prozac Reduction Timeline
I would really like to thank Alto Strata at http://survivingantidepressants.org/ who asked a knowledgeable doctor about what was happening to me and the conclusion was that by going to 1.05ml I may have overshot my bolt, and the Prozac was becoming too activating, it is a stimulating drug and I seem to be very sensitive. When we studied it I was beginning to feel better shortly after I went to 1.05ml but since Prozac takes a lot of days to reach “high tide” it was probably the effect of going up to 1ml beginning to take effect and then I ramped it up by going up further to 1.05ml and got worse again. So I’m going to see how back to 1ml goes.
In my real life I seem to be surrounded by people who just “stopped” their drug or had no problems, I am so thankful for the internet and finding that I’m so NOT alone with this and I'm not mad.

My Prozac Reduction Timeline
Saturday, 17 November 2012
1.05ml - Arresting the Spiral
 So I’ve found myself
spiralling down in a way that I hadn’t felt for 5-6 years, after years of
fairly benign withdrawals because I’ve been tapering so slow, I was shocked to
find myself getting all the old symptoms from years back. A bad withdrawal
seems to take your most negative emotion like anxiety and ramp it up or amplify
it to a spirit crushing level. Mind you depression does that as well?!?!
So I’ve found myself
spiralling down in a way that I hadn’t felt for 5-6 years, after years of
fairly benign withdrawals because I’ve been tapering so slow, I was shocked to
find myself getting all the old symptoms from years back. A bad withdrawal
seems to take your most negative emotion like anxiety and ramp it up or amplify
it to a spirit crushing level. Mind you depression does that as well?!?!
As
I’ve documented in the posts below the worst things I was getting and still
getting on and off, was insomnia, deep despair, dread and adrenaline/anxiety. I
actually, maybe naively, thought I’d left those things behind years ago in the
bad old days. It’s impacting on my life again recently in ways I hate; I’ve
been too exhausted to go into work for a few days during October/November, and
I’m struggling to get myself back on an even keel again. Insomnia is the most debilitating symptom and just
aggravates everything else and is classic in drug withdrawal.
So having taken guidance from the eminently knowledgeable
and wise Alto Strata, (who I probably should have listened to months ago when
she suggested a micro taper to me)
I’m going to go up a tiny bit more to 1.05ml in an extra bid to clear my
current issues, as she explained it .05 is 5% of 1ml and it could well be that
I am sensitive to tiny amounts now, and Prozac is a stimulating drug, if I’m
sensitive I don’t want to aggravate things further but need to find the right
balance and stabilise myself at that point.
So I suppose the lesson here is never get blasé and
underestimate the power of these drugs, for good or bad depending on how you
view them.
The other lesson is that recovery and progress doesn’t
always happen in a straight line.
Saturday, 10 November 2012
1ml (4mg) - A Small Reinstatement
So on Wednesday I had to updose a tiny bit back to 1ml, the received wisdom from those who have trod this path before me is that if you start unravelling it's best to go back to the dose where you last felt well, so this is what I've done, I will write more fully about it hopefully in the next week, right now I'm just totally drained.
Prozac Reduction Timeline
Prozac Reduction Timeline
Monday, 29 October 2012
C'mon Inner Peace I Don't Have All Day!!
The people who mentioned it gets hard near the end, they were not wrong!! Anyway I realised this blog was turning into
a right misery pity fest so I want to turn it around again into a more positive story
of recovery and celebrate the fact that I have in fact come a long long way
even if there is still a bit or work to do.
I’m getting the adrenaline surges I used to get years ago when I did cold turkey but not as severe, it becomes a bit of a downward spiral because adrenaline surges means it’s hard to relax/sleep and in turn the tiredness/exhaustion makes the surges feel worse and more desperate; the one positive thing about adrenaline surges is that they appear to eat calories and I can now eat cake and lose weight.!!Has to be some benefit doesn’t there? Yesterday I had a couple of strong coffees in the morning and couldn’t help but notice how very on edge I felt an hour or so later, so I guess that’s something I’ll have to cut down or eliminate, hopefully temporarily. I have taken some advice and this is the positive action I am taking:
Out with the bungee jumping
Out with the trips to Alton Towers, no more Oblivion for me, at least for the time being
 And:
And:
Replace tea and coffee with chamomile, green and rosehip tea (boring but soothing)
I’ve been trying to unravel whether this is “withdrawal”
or mind and body rebelling against the crutch I’ve had for so
many years now disappearing, and even whether I ought to up dose a bit or tough this out. At the moment I’m going to stay at this dose, take positive action as above and mull over how to proceed in the
future.

I’m getting the adrenaline surges I used to get years ago when I did cold turkey but not as severe, it becomes a bit of a downward spiral because adrenaline surges means it’s hard to relax/sleep and in turn the tiredness/exhaustion makes the surges feel worse and more desperate; the one positive thing about adrenaline surges is that they appear to eat calories and I can now eat cake and lose weight.!!Has to be some benefit doesn’t there? Yesterday I had a couple of strong coffees in the morning and couldn’t help but notice how very on edge I felt an hour or so later, so I guess that’s something I’ll have to cut down or eliminate, hopefully temporarily. I have taken some advice and this is the positive action I am taking:
Out with the trips to Alton Towers, no more Oblivion for me, at least for the time being
Cut down on tea and coffee
Eat healthy
Magnesium citrate (was already taking magnesium but apparently magnesium citrate is much better absorbed and is good for the nervous system and muscles)
Melatonin (good for sleep)
Learn about Mindfulness, “Wherever You Go There You Are” on order.
Keep up with the exercise, sadly weather for cycling is not good but I still have the X trainer.
Continue to appreciate my caring and supportive husband who worries about me, and my funny affectionate sons.

Sunday, 28 October 2012
Peter Hitchens writing in the Daily Mail about Felicia Boots
Peter Hitchens often writes on this topic in the Daily Mail. I have actually been avoiding this story because it's really so painful, but it is actually really important to share this, as most people will be missing the point entirely and blaming the post natal depression, the real story is that she stopped taking her pills cold turkey. Thank you thank you Peter Hitchens.
As soon as I learned that she had killed her own children and then tried to do away with herself, I was sure that I would find she had been taking ‘antidepressants’. And so it proves.
Our courts let many people off because of spurious claims that they could not control themselves.

But I believe that in her case the judge was right to say that this unhappy woman was in the grip of ‘forces that were beyond her control’.
It will be pointed out that she had recently ceased taking these pills, because of a perfectly reasonable fear of passing on the drugs to her children through her breast milk.
To anyone who has studied the matter, the fact that Mrs Boots became unhinged after ceasing to take her ‘antidepressants’ will be no surprise.
Normal human beings become abnormal, possibly for ever, as soon as they first ingest these powerful, poorly-researched chemicals, often prescribed by doctors shamefully ignorant of the growing body of expert criticism of them.
The effects of coming off them can be even worse than the effects of starting to take them. I have absolutely no personal stake in this argument. I have simply observed what seems to me to be a pattern, both among several people known to me and in a growing number of news reports.
I will be told this is ‘anecdotal’. Very well, then. Let us have a proper, fully-funded inquiry that will settle the matter once and for all. It is very urgent. Prescriptions of ‘antidepressants’ grow all the time.
If there is the slightest risk that they make good, kind mothers lose their minds and kill their own babies, I can imagine few more pressing matters on the agenda of any government than to establish the truth and act on it. Please, somebody listen.
Link to the article (scroll down)
Investigate the evil of these pills
I bit my tongue when I first read of the tragedy of Felicia Boots, her life now a desolation of unbearable grief.As soon as I learned that she had killed her own children and then tried to do away with herself, I was sure that I would find she had been taking ‘antidepressants’. And so it proves.
Our courts let many people off because of spurious claims that they could not control themselves.
Probe: Peter Hitchens wants an inquiry into the usage of antidepressants following the tragic story of Felicia Boots, right
It will be pointed out that she had recently ceased taking these pills, because of a perfectly reasonable fear of passing on the drugs to her children through her breast milk.
To anyone who has studied the matter, the fact that Mrs Boots became unhinged after ceasing to take her ‘antidepressants’ will be no surprise.
Normal human beings become abnormal, possibly for ever, as soon as they first ingest these powerful, poorly-researched chemicals, often prescribed by doctors shamefully ignorant of the growing body of expert criticism of them.
The effects of coming off them can be even worse than the effects of starting to take them. I have absolutely no personal stake in this argument. I have simply observed what seems to me to be a pattern, both among several people known to me and in a growing number of news reports.
I will be told this is ‘anecdotal’. Very well, then. Let us have a proper, fully-funded inquiry that will settle the matter once and for all. It is very urgent. Prescriptions of ‘antidepressants’ grow all the time.
If there is the slightest risk that they make good, kind mothers lose their minds and kill their own babies, I can imagine few more pressing matters on the agenda of any government than to establish the truth and act on it. Please, somebody listen.
Link to the article (scroll down)
Saturday, 20 October 2012
Cutting Up Rough

Just had one of the worst few days in a long while, since I embarked on this taper in 2008 my withdrawals have been fairly benign and I’ve been pretty much able to work through them. This time however I’ve had a few days that have felt much more crippling in intensity, I’m wondering if it’s because now I’m below 1ml each cut I make is more than 10% of previous dose. At this point I could make micro cuts, which could be endless, or just leave even longer between cuts and accepting that the withdrawals will be more debilitating when they do hit. At the moment I am thinking the latter; whatever, it’s just really frustrating to be so near and yet so far to the end. It’s so tempting to just think to hell with it and just drop this last bit dead but I just know Prozac and my brain won’t like it and will cut up very rough.
These past few days I’ve had the following:
·
Wired/caffeinated feeling
·
Insomnia (one night I got so fed up I went
downstairs and made a packed lunch and sorted laundry, went back to bed and
still couldn’t sleep)
·
Free floating anxiety
·
Crying
·
Despair
At my lowest point I nearly deleted my page off Facebook and
this blog, until P talked me out of it, and now I’m so glad I didn’t, I would have missed the page and all the
wonderful people out there. This time I even had to take a couple of days off my local authority job and I
felt really bad about that, I’m so used to rarely being off sick. The plus side
is that I work with a great team of people, and I felt able to tell the truth
about why I was off sick and even had a lengthy chat about it with a colleague
when I did get back and it was all positive.
Today I feel like I’m definitely coming out the other side
and I’m just left feeling like I’ve been through the wringer and feeling a bit
spaced out.
I do just want to address something that I know people think
but are too polite to say or ask, everyone who goes on these drugs went on them
for a reason, depression, anxiety (and nowadays PMT, ADD, ADHD, physical pain or any number of different
ailments). How do I know I’m not just depressed still? Of course I’m not naive
enough to think depression will leave my life forever, of course I will always
be someone prone to depression/anxiety as part of my makeup and I am ever
mindful of that fact. Having had depression I know that with no drugs involved
it just doesn’t shift that quickly, it’s a longer haul. When doing a slow taper
off a drug the depressions are mercifully time limited and do shift in a way
that depression wouldn’t.My youngest son is 14 this coming week, this means its 14 years since this story started.
I just want to end this post with a picture made by a good friend Paul:
Wednesday, 10 October 2012
Today is World Mental Health Day

A portion of the proceeds of the event are going to Suffolk Mind and The Mind Sanctuary in Suffolk. This was too good an event for us to miss as it combines business networking for P and mental health awareness which is of interest to us both.
The Mind Sanctuary
Suffolk Mind
Saturday, 6 October 2012
Antidepressant Withdrawal is Hell!
When I shared this picture on my Facebook page a while back I was shocked by how much response it got, so many related to it or had something to say about it.
I could tick at least half the things on that list and many people I know could tick nearly all.

Monday, 1 October 2012
It's.just.a.drag
So a week into my tiny cut this is how I've been feeling, my sleep pattern has temporarily gone to pot and I've been dragging my weary ass through the days, it's. just. a. drag. On saturday I'd had a good nights sleep but despite that I just felt like someone had pulled my plug out, I felt drained like when you have flu. No emotionals this time, just tiredness, I know it will pass. I really was hoping to speed up the last bit of the taper now, but P, very sensibly said what does it matter? who cares if the last bit takes another load of months? enjoy the stability in between the drops? I know he's right darn it!!
Prozac Reduction Timeline
Sunday, 23 September 2012
0.85ml and Surviving Antidepressants
It's been a long time since my last reduction, I decided to hold it steady over the summer as I did feel the last cut for a while, and it took me a bit by surprise. Now I'm on the home stretch I decided to make smaller cuts as the last bit is allegedly the hardest. Partly at the suggestion of Alto Strata on the Surviving Antidepressants web site and partly because my husband worries :)
 Speaking of Surviving Antidepressants I was hugely flattered a few weeks ago when I got a message from Alto Strata at Surviving Antidepressants asking me if I would like to help admin/moderate the forums and in particular the "Tapering" forum. I was impressed with my "staff" badge on the site, but at first I wondered what I let myself in for, not because I was worried about talking/helping people on the forums, I do that a lot anyway, it was more all the techy bits I now have access to behind the web site. I also wondered if I would be able to do it justice and visit the site enough to keep up with people, but it's been absolutely fine and the tapering forum doesn't move as fast as some of the others forums on the site.
Speaking of Surviving Antidepressants I was hugely flattered a few weeks ago when I got a message from Alto Strata at Surviving Antidepressants asking me if I would like to help admin/moderate the forums and in particular the "Tapering" forum. I was impressed with my "staff" badge on the site, but at first I wondered what I let myself in for, not because I was worried about talking/helping people on the forums, I do that a lot anyway, it was more all the techy bits I now have access to behind the web site. I also wondered if I would be able to do it justice and visit the site enough to keep up with people, but it's been absolutely fine and the tapering forum doesn't move as fast as some of the others forums on the site.
Link to Surviving Antidepressants for Anyone Seeking Support
Link to Surviving Antidepressants for Anyone Seeking Support
Friday, 10 August 2012
Prozac Taper Progress Report
So here I am still at 0.90ml since mid June. It’s not been
an easy ride this time; I had a feeling from things I’ve heard from other
people that it can get tricky when you get near the end. I’ve been waking up
with low level depression, waves of sadness most mornings, sometimes it hangs
around like a bad smell for best part of the day, but mostly it does dissipate
mid morning. That’s it, it’s just low level and niggling, not crippling. It has
crossed my mind that either I could get stuck at this low dose, permanently, or
the last 1ml of the taper could just take an awful long time. It’s the sheer
subtlety of it now, the not knowing what it is that’s really annoying, is it
withdrawal or “me”? I do know that I am always going to be one of those people
who will be “prone” to depression and anxiety and therefore I need to be mindful.

Prozac reduction timeline
This happened to a fellow taperer/friend (I hope she doesn’t
mind me mentioning) and she reluctantly chose to stay at the very low dose
permanently because every time she dipped below that level depression kicked
in. As she said “it is what it is”. It’s great to compare notes with someone
else from a completely different country and different walk of life but going
through the exact same thing.
In the meantime, I am helping a lady in New Zealand to admin her support group on Facebook, there are about 90 people in the group, not all active, I think some just like to sit quietly and read things. It's a brilliant supportive and friendly group so if anyone reading this and needs help/advice and would like to join please contact me and I'll add you, it is a closed group, not visible unless you search for it, and therefore no one outside the group can read anything in it.

Today is a good day though, the sun is shining, I now have 2
weeks off from my part time job (not from helping Peter with the business
though sadly), we are going to a Newmarket Race Night this evening with some very good friends, Tom Jones will be performing at the end of the races, and over the next two weeks I’ll get to
spend more time with my youngest and catching up with friends before the new
school term starts.
Prozac reduction timeline
Saturday, 21 July 2012
School Shootings, SSRI Nightmares, Suicide and Violence
 I don't normally dwell TOO much on the dark side on my blog, partly because I want it to be a story of recovery, but there is a massive dark side which can't be ignored. Back in 1999, 2000, 2001 I would have dismissed it as scaremongering bollox as well.
I don't normally dwell TOO much on the dark side on my blog, partly because I want it to be a story of recovery, but there is a massive dark side which can't be ignored. Back in 1999, 2000, 2001 I would have dismissed it as scaremongering bollox as well.
Until I experienced it myself I never would have believed it. Cold turkey sent me to a very very dark place, by end of 2003, I knew I couldn't go on much longer, it was harder and harder to keep a front up, at work and at home, the only person who really knew what was going on was my husband, I couldn't eat properly, I couldn't sleep, I couldn't stop the adrenaline surges day and night, I couldn't stop the dark dark thoughts and feelings. The adrenaline surges were the hardest thing to deal with. If you can imagine the gut churning fight or flight response never switching itself off. I couldn't tell anyone, people talk about "losing the plot" but I really had lost the plot and was lost in my own inner torment that no one could see, let alone understand. Hell I didn't understand it myself so how would anyone else? I did get to a point where images of the Orwell Bridge entered my head, it was just a thought but it was there. I've since met people who've had similar experiences with coming off too fast, severe agitation, distressing thoughts of violence towards other people and themselves, which cleared with reinstatement of the drug. This happened again to me in 2005, 2006 and 2007 but to a much lesser degree as I reinstated the drug more rapidly when I realised what was happening.
If I had perservered without reinstating Lustral for another month or so into 2004, I think the internal agitation, desperation and despair would have driven me to something dreadful to end the misery. Fortunately with my husbands encouragment I reinstated Lustral and fairly swiftly my symptoms subsided. This was my insight into the dark side of SSRI's.
No one told me this could happen.
Since writing this blog I've met many others with similar experiences and I've read a lot. Really I do need to get a life, but knowing the medical establishment are either genuinely ignorant or totally in denial and there is so little help out there, I am prepared to talk about it here knowing that others stumble on it and find they are not alone.
Sometimes even now when I drop my dose I get a flavour of that "dark side" again for a few days, and then it just suddenly disappears as my brain/body gets used to the new slightly lower level of Prozac. My husband is so finely tuned into me, he knows, he said to me the other week I looked like I had the weight of the world on my shoulders, and then almost overnight it just went as my metabolism adjusted to the new lower dose.
In recent years as I've done a lot more research into SSRI's I've discovered my experience wasn't unique, but many many people when it happens don't know the inner agitation/adrenaline surges is a side effect of dropping a drug too fast. Suicide and violence are now recognised in many circles as side effects of dropping Prozac/Lustral/Seroxat etc too fast, or starting it too fast.

SSRI stories This is a really interesting data base of reported SSRI related violence/suicide, there is even a celebrity section.
Many many stories of random violence or suicide that you read in the media have an underlying hidden story of prescription medication behind them that the media generally don't pick up on, unless it's a celebrity, maybe. Unless you've experienced it yourself it just doesn't cross your mind.
Hmm I can hear some people I know reading this and thinking, yes, but how do you know it's the drug? you might be a sandwich short of a picnic and the drug might be nothing to do with it, how do you know it's not the mental illness? well that's the head f*** because it can always be blamed on the original illness and big pharmaceutical companies hide behind this.
But don't just take my word for it, look at SSRI stories and Dr David Healy, professor of psychiatry in Wales.
Sunday, 8 July 2012
The best way out is always through
Following on from last weeks post, I am now coming out the other side, I've had about 10 days to 2 weeks of:
My Prozac reduction timeline
- Low level depression/anxiety, worse first thing, better as day goes on
- Poor sleep
- Fuzzy head, worse when tired, which has been a lot
My Prozac reduction timeline
Sunday, 1 July 2012
Going through a withdrawal
That's it, I know I'm going through a withdrawal, my head has been a bit spaced out all week, I've been up and down and just "not quite right", anxiety has kicked in, I've had those feelings of fear that it won't go away, but I've done this so many times before now, I know it will go away again. This too will pass.


Saturday, 16 June 2012
0.90ml - and Low blood sugar
 So now I've broken the 1ml barrier! I've always suffered with low blood sugar, even before I went on Sertraline, but I know it is also aggravated by SSRI's, I wonder if this is the reason why many people gain weight and it's a known side effect of these drugs. Lately it just seems to be really bad, mornings are worst for me, half way throught he morning I'm already hungry and my mid day I'm ravenous and if I don't get my lunch I am all those things in the picture to the right! and if lunch is not adequate enough by mid afternoon I have a real thumping headache. I am experimenting now with cutting out sweets, biscuits, cakes, puddings to see if that helps, not that I eat a lot of cakes but I naturally crave sweet stuff when I see it. I thought about cutting out tea/coffee as caffeine is known to aggravate it, but that lasted all of about two days!! I manage to keep my weight in the range it should be but it's a struggle. Hence the bike rides/exercise. Anyway, I am curious to know if this is an issue for anyone else? and how you deal with it?
So now I've broken the 1ml barrier! I've always suffered with low blood sugar, even before I went on Sertraline, but I know it is also aggravated by SSRI's, I wonder if this is the reason why many people gain weight and it's a known side effect of these drugs. Lately it just seems to be really bad, mornings are worst for me, half way throught he morning I'm already hungry and my mid day I'm ravenous and if I don't get my lunch I am all those things in the picture to the right! and if lunch is not adequate enough by mid afternoon I have a real thumping headache. I am experimenting now with cutting out sweets, biscuits, cakes, puddings to see if that helps, not that I eat a lot of cakes but I naturally crave sweet stuff when I see it. I thought about cutting out tea/coffee as caffeine is known to aggravate it, but that lasted all of about two days!! I manage to keep my weight in the range it should be but it's a struggle. Hence the bike rides/exercise. Anyway, I am curious to know if this is an issue for anyone else? and how you deal with it?
But anyway! 0.90ml!!!! A friend on facebook said there would be a party on facebook when I make it to 0. No pressure then!
Friday, 15 June 2012
Mind - Making sense of coming off psychiatric drugs
I discovered last week that Mind, the mental health charity in the UK, have a really really good page on their web site about coming off psychiatric drugs. You can either read it on line and print it off or you can send off for it as a booklet for £2. Perhaps it would be a good idea for people to print off and give to their doctors! There is also another booklet called "Coping with coming off" which is £2 but no idea what it's like, you have to send off for that one to read it.
Mind - Making sense of coming off psychiatric drugs

Mind - Making sense of coming off psychiatric drugs
Monday, 4 June 2012
Hanging in There
I had really hoped that I would be going to 0.90ml this week end, but, I went down with tonsillitus, been feeling generally really run down physically, ear ache, head ache and as well my head is feeling just so, how can I describe it? just kind of dizzy which I know is a side effect of withdrawal. So, my mentor (Peter) has told me sensibly to hold off another week or maybe two.

Saturday, 26 May 2012
4th Anniversary
 Today is the 4th anniversary of my taper, I made my first timid reduction to 4.90ml on 25th May 2008, I'd switched to liquid Prozac in the February and in fact Peter wanted me to wait until about August before starting my taper because we were rennovating the house and it was in chaos, but I was a bit impatient and in fact that first reduction was me allowing a little air bubble in the syringe as a cautious experiment. In fact it was more like 4.95 than 4.90, that's how scared and phobic you get about it. Now I WAS going to go down to 0.90ml today, but, this week my sleep pattern has been shot to bits and I am decidedly cranky so I'm going to leave it another week.
Today is the 4th anniversary of my taper, I made my first timid reduction to 4.90ml on 25th May 2008, I'd switched to liquid Prozac in the February and in fact Peter wanted me to wait until about August before starting my taper because we were rennovating the house and it was in chaos, but I was a bit impatient and in fact that first reduction was me allowing a little air bubble in the syringe as a cautious experiment. In fact it was more like 4.95 than 4.90, that's how scared and phobic you get about it. Now I WAS going to go down to 0.90ml today, but, this week my sleep pattern has been shot to bits and I am decidedly cranky so I'm going to leave it another week.One thing I have been getting is a lot more of the dizzy head feeling, I think because up to recently I have never dropped more than 10% of previous dose but now I am so low, if you do the maths the drops as a percentage of the previous dose get steeper so I think my head is feeling it now. I never had the brain zaps that other people describe, more of a dizzyness and waterlogged fuzz inside my head.
Oh and this week Bobby Fiddaman asked me and another person to write guest blogs on SEROXAT SUFFERERS - STAND UP AND BE COUNTED about sertraline (zoloft), I said yes but I don't know what to write, how mad is that?!?! I've been blathering on here about it for four years and found enough to say!!
Anyway, as it's my 4th anniversary here's my timeline for the past four years, just in case you haven't already seen it ;)
I think by this time next year I'll be done.
25th May 2008 4.90ml
10th June 2008 4.80ml
14th July 2008 4.70ml
14th Aug 2008 4.60ml
14th Oct 2008 4.50ml
25th Nov 2008 6 months
3rd Dec 2008 4.40ml
24th Jan 2009 4.25ml
11th April 2009 4.10ml
18th April 2009 3.90ml
17th May 2009 3.80ml
25th May 2009 1 Year
6th July 2009 3.60ml
22nd Aug 2009 3.50ml
2nd Oct 2009 3.30ml
14th Nov 2009 3.20ml
25th Nov 2009 18 Months
24th Dec 2009 3.10ml
31st Jan 2010 2.90ml
6th March 2010 2.70ml
10th April 2010 2.60ml
25th May 2010 2 Years
5th June 2010 2.50ml
3rd July 2010 2.40ml
7th Aug 2010 2.30ml
18th Sep 2010 2.20ml
23rd Oct 2010 2.00ml
25th Nov 2010 2 Years 6 months
18th Dec 2010 1.90ml
2nd March 2011 1.80ml
28th April 2011 1.70ml
25th May 2011 3 Years
10th June 2011 1.60ml
23rd July 2011 1.50ml
10th Nov 2011 1.40ml
25th Nov 2011 3 Years 6 Months
18th Dec 2011 1.30ml
17th Feb 2012 1.20ml
26th March 2012 1.10ml
28th April 2012 1.00ml
25th May 4 Years
1ml syringe

Tuesday, 1 May 2012
It's not where you are in life, it's who you have by your side that matters
So I've definately been getting this effect today. Earlier when I was looking at a book or a screen I felt like there was a wodge of cotton wool between my brain and what I was trying to take in, hard to describe, but nowadays it's not too bad compared to how it used to be a few years ago, I guess it's the brain adapting to firing on it's cylinders with less of the drug.

In fact I commented to P today on how transient the withdrawals are now, that sometimes I forget how rubbish it was a few years ago and feel a bit of a fraud now with my blog and facebook page, his response; you're not a fraud, you may forget sometimes but I bloody don't!!
It reminds me how dreadful it was for him as well, scary for him living with me slowly cracking up and neither of us talking to anyone outside of us about it, and while I was preoccupied with struggling with waives and waives of sadness and anxiety washing over me with the occaisional glimmer of light which I held out for, but which was always dashed with more waives of sadness, he was also struggling, with his own confusion and fears. Depression/SSRI withdrawal can make a person appear pretty damned selfish and preoccupied and frustrating and hard for partners to deal with, not sure I could have dealt with it had the boot been on the other foot, I married a real gem.
Friday, 27 April 2012
1ml of Prozac and the man from Pakistan
Now down to just 1ml, so glad to get rid of that pesky .1 of a ml
 I am part of a really nice group on facebook about 50 of us, different stages of tapering off SSRI's mostly Seroxat but one or two others like me. Most of us are from US, UK and New Zealand, the group had been pretty quiet and not a lot going on, but recently Adnan Abid from Pakistan
I am part of a really nice group on facebook about 50 of us, different stages of tapering off SSRI's mostly Seroxat but one or two others like me. Most of us are from US, UK and New Zealand, the group had been pretty quiet and not a lot going on, but recently Adnan Abid from Pakistan burst on the scene joined our group, his English is pretty good, he had so much to learn about how to come off Seroxat and the group really came into it's own with the help and moral support, and humour, it was like he was the catalyst to really get the group talking, and what a nice group it's turned out to be, just a shame we're all so far flung and can't all meet up.
I don't normally mention people by name on here, to protect their privacy, but Adnan was so thrilled I'd mentioned him he asked me to edit this and mention him properly by name, so here it is Adnan!
My Prozac Reduction Timeline
 I am part of a really nice group on facebook about 50 of us, different stages of tapering off SSRI's mostly Seroxat but one or two others like me. Most of us are from US, UK and New Zealand, the group had been pretty quiet and not a lot going on, but recently Adnan Abid from Pakistan
I am part of a really nice group on facebook about 50 of us, different stages of tapering off SSRI's mostly Seroxat but one or two others like me. Most of us are from US, UK and New Zealand, the group had been pretty quiet and not a lot going on, but recently Adnan Abid from Pakistan I don't normally mention people by name on here, to protect their privacy, but Adnan was so thrilled I'd mentioned him he asked me to edit this and mention him properly by name, so here it is Adnan!
My Prozac Reduction Timeline
Sunday, 15 April 2012
I Like to Know Things!
This is a 10 minute clip, and Shannon really amuses me. I think my tongue is in my cheek posting this one, you have to get past the very short skirt, the cliche sexy librarian look, and the Texan accent (sorry American friends) and if you really close your eyes and actually listen to what Shannon is saying about critical thinking with particular reference to antidepressants and the chemical imbalance theory, you get a basic lesson in how to look at advertising and think critically about how things are worded.
This Youtube clip is from Psychetruth website and here Psychetruth on Facebook.
They do a whole series of Youtube clips on lots of different health topics but I really don't know what their credentials are, whether they are doctors, scientists or everyday people doing research?
Prozac Reduction Timeline
Thursday, 5 April 2012
2 Weeks? Try 12 years!!!!
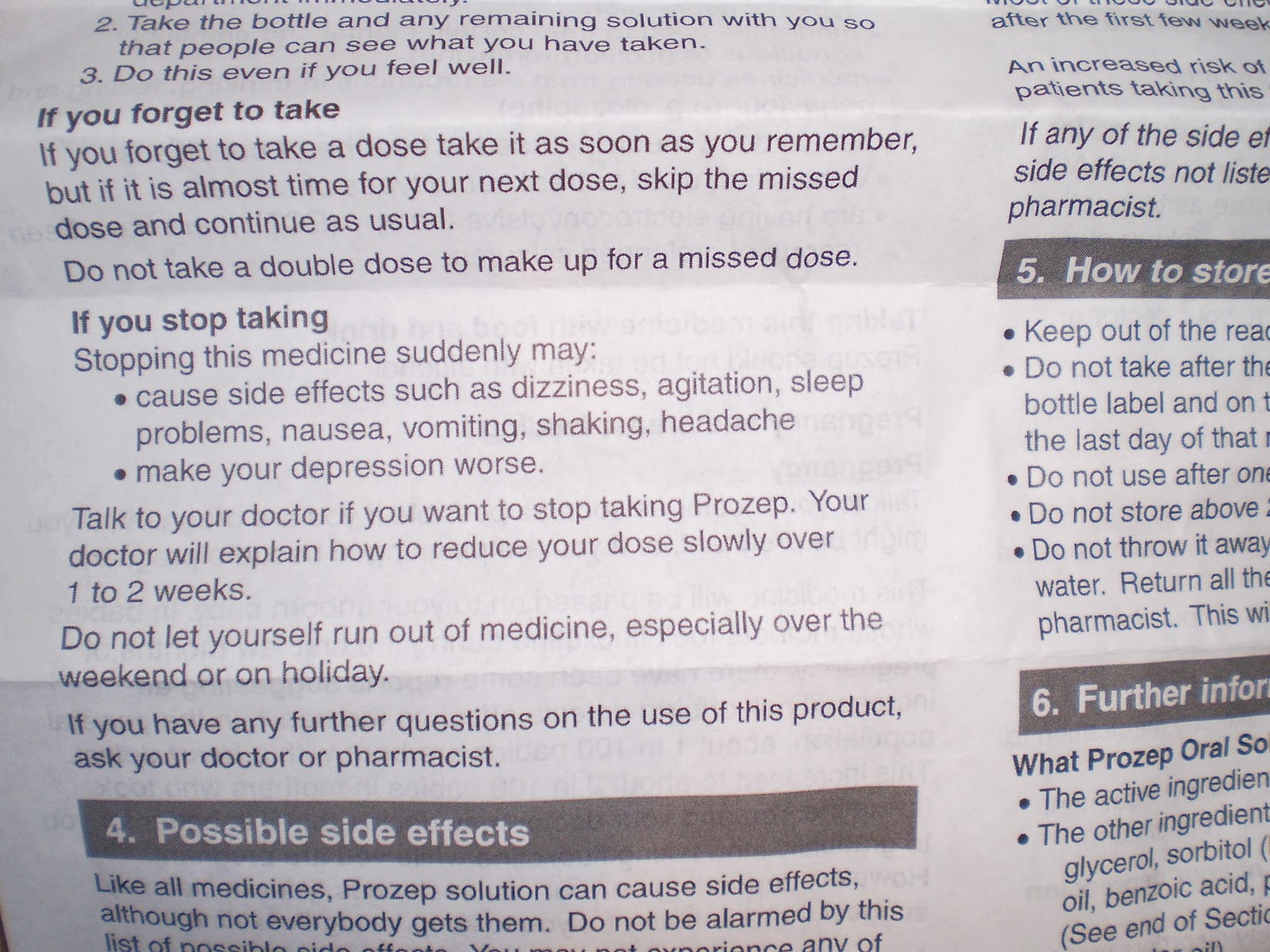
Anyway, I got my prescription, and when I got in the car I looked at the patient info leaflet for the first time in a long long time, and I just had to photograph it and put it on here, can you see?? it tells you a few side effects if you stop taking this medicine suddenly, but then it tells you to talk to your doctor if you want to stop taking Prozep (the Prozac I have is called Prozep for some reason) and your doctor will explain how to reduce your dose slowly over 1 to 2 weeks!!!!!!!!!!
At the start of Jan 2007 I was on 5ml Prozac and I started reducing by 0.10ml a week, by February half term week the bottom was well and truly dropping out of my world again, adrenaline surges, insomnia, extreme restlessness, profound sadness/depression, and no this wasn't the depression returning, it was much more physical than that.
If this is the information patients and doctors are getting is it any wonder so many people including doctors are so confused??!!??
Prozac Reduction Timeline
Sunday, 25 March 2012
1.10ml
 Going down to 1.10ml today. I keep being asked if I'm noticing it getting any harder now I'm right down low on the dose, and I have to say the only thing I'm noticing I'm getting a lot more of is the dizzy head, sometimes it's like my head is packed with cotton wool and it's hard to get a handle on a particular thought, it's only a minor thing and I suspect it will just come and go with time, so if you ask me a question and I give you a blank look it might be that I'm processing it through the cotton wool (that's my excuse anyway!).
Going down to 1.10ml today. I keep being asked if I'm noticing it getting any harder now I'm right down low on the dose, and I have to say the only thing I'm noticing I'm getting a lot more of is the dizzy head, sometimes it's like my head is packed with cotton wool and it's hard to get a handle on a particular thought, it's only a minor thing and I suspect it will just come and go with time, so if you ask me a question and I give you a blank look it might be that I'm processing it through the cotton wool (that's my excuse anyway!).I've had some lovley e mails from people who've read my blog, I've said it loads of times before but it really does make my day when someone takes the trouble to write to me and tell me they got something out of reading my waffle on here!
Prozac Reduction Timeline
Saturday, 24 March 2012
Liebster Award
I've had a really nice surprise, I got nominated for a Liebster blog award by The Highly Unlikely Housewife, first time I've had a blog award, so thank you! I have no idea what Liebster means, but anyway here are the rules of engagement for this award:

- Thank the person that nominated you on your blog and link back to them.
- Nominate up to five other blogs for the award.
- Let them know via a comment on their blog.
- Post the award on your blog.'

As I understand it this award is for blogs with less than 200 followers, so here are my nominations:
No Spend Days because I love reading her thrifty blog and I aspire to be more thrifty myself but don't always suceed.
Maithancailin because she is my best friend, she writes brilliant poetry and is naturally a much better writer than I could ever hope to be, and I hope she puts some poetry on her blog soon.
Crazy People Music because I like his music, and because he has been really supportive of my blog/taper and he is good company on facebook.
Everyones Gran because she is funny and entertaining and been a great support as well.
Struggling With the Elephant in the Room Manic Depressive Blog because David has written a really eloquent blog about his personal struggles with mental health issues, but he has been really very unwell lately and I miss his blog posts, and I'm kind of hoping this might help him get back to his writing, but if nothing else just to let him know that people do care.
Sunday, 26 February 2012
Numb Documentary - Watched at Last
 |
| Numb website - order the documentary here
I watched this last night, that was a big mistake, my sleep pattern has been a bit shot lately and watching this before bed didn't help!
It was absolutely spot on and I related to ALL of it. I've written about what it feels like to stop taking your antidepressant and what happens Akathisia as have many others, but Phil has gone a step further and actually filmed what happened when he halved his antidepressant. There's no way I wanted anyone to see me in that state and I actively hid myself and "it" when the withdrawals kicked in. Big kudos to Phil for doing this.
The excerpt with his very supportive wife was exactly how Peter was with me, especially where she said she didn't want Phil reading the worst case scenarios on the internet, it was obvious to me Phil was reading the Paxil Progress web site, exactly as I had when desperately searching for the answers. The impact on marriage and family life was an exact mirror image of ours when I was trying to stop taking my antidepressant. Peter on the outside trying to understand what was going on but feeling pretty helpless. Phil tried everything I tried, diet, exercise, alternative remedies, all to no avail. In the end he did what I had to done so many times, he restarted the antidepressant, after much angst and wrestling with whether to persevere with his withdrawals or give in and go back to the drug. I was interested to see he switched to Prozac, just as I did, and I wonder if it was with a view to attempting to taper off liquid Prozac in the future.
Something else jumped out at me, one commentator in the documentary talked about whether these drugs are "addictive" or not, and this is a question that I have wrestled with. The commentator (I can't remember who it was, perhaps someone will remind me) made the point that the drug companies tell you they are not addictive because you don't see people selling them on street corners and people craving them, but that's because it's so easy to get your prescription filled from the doctor. I have sat in the surgery and heard someone begging for a doctors appointment because they hadn't realised they'd run out of their seroxat and if they didn't get it they would be in a terrible state the next day.
If anyone around me wants to borrow it and watch please feel free to ask me, but I won't post it to anyone because I don't want to risk losing it!
|
Tuesday, 14 February 2012
1.20ml - New Reduction
It's been two months since I last reduced, I think I'm deliberately taking it slower over the winter.
 I've said it before and I'll say it again but I'm at a stage where it would be so easy to just stop taking the Prozac, I'm on such a stupidly low dose, but on the other hand I'm scared of all my hard work and patience unravelling at the end. So I'm keeping in mind what I read that I shouldn't ever reduce more than 10% of the last dose I was on, and when you think about the maths, the lower I go, the steeper the % drops.
I've said it before and I'll say it again but I'm at a stage where it would be so easy to just stop taking the Prozac, I'm on such a stupidly low dose, but on the other hand I'm scared of all my hard work and patience unravelling at the end. So I'm keeping in mind what I read that I shouldn't ever reduce more than 10% of the last dose I was on, and when you think about the maths, the lower I go, the steeper the % drops.
So I'm really not sure how this will work when I hit 1ml, I think I may have to consider when my jumping off point will be.
NEVER underestimate how this class of drug can screw you up. I'll carry on being the tortoise and not the hare for the time being.
My tortoise Prozac reduction timeline!
 I've said it before and I'll say it again but I'm at a stage where it would be so easy to just stop taking the Prozac, I'm on such a stupidly low dose, but on the other hand I'm scared of all my hard work and patience unravelling at the end. So I'm keeping in mind what I read that I shouldn't ever reduce more than 10% of the last dose I was on, and when you think about the maths, the lower I go, the steeper the % drops.
I've said it before and I'll say it again but I'm at a stage where it would be so easy to just stop taking the Prozac, I'm on such a stupidly low dose, but on the other hand I'm scared of all my hard work and patience unravelling at the end. So I'm keeping in mind what I read that I shouldn't ever reduce more than 10% of the last dose I was on, and when you think about the maths, the lower I go, the steeper the % drops.So I'm really not sure how this will work when I hit 1ml, I think I may have to consider when my jumping off point will be.
NEVER underestimate how this class of drug can screw you up. I'll carry on being the tortoise and not the hare for the time being.
My tortoise Prozac reduction timeline!
Monday, 13 February 2012
Psychiatric Drug Withdrawal: Why Taper by 10% of your Dosage?
I found this today and thought it was an excellent article, I have also put it as a page on the side for reference. It's more or less the method I've been following. Just been wondering where my "jump off" point will be....
By AltoStrata
AltoStrata's Surviving Antidepressants Web Site
Why taper by 10% of my dosage?
 Many people seem to be able to taper off psychiatric medications in a couple of weeks or even cold-turkey with minor withdrawal symptoms perhaps for a month or so. Doctors therefore expect everyone can do this. However, it seems a minority suffer severe symptoms for much longer.
Many people seem to be able to taper off psychiatric medications in a couple of weeks or even cold-turkey with minor withdrawal symptoms perhaps for a month or so. Doctors therefore expect everyone can do this. However, it seems a minority suffer severe symptoms for much longer.
It is unknown how large or small this minority is. You may very well be in it. You cannot know how your nervous system will respond to a decrease in medication until you try it.
Withdrawal symptoms represent neurological dysfunction. Severe symptoms can be distressing, debilitating, or even disabling. If you get prolonged withdrawal syndrome, there is no known treatment or cure. You will have to cope with it until it goes away.
Some guides will suggest a trial decrease of 25% to start. If you get withdrawal symptoms, it is recommended to reinstate the original full dosage and taper more slowly from there.
That is reasonable, except that it can take weeks to feel the full brunt of withdrawal symptoms from an initial drop. If you have already made two reductions from your original dosage, you will have reduced by about 50% — and your symptoms may indicate substantial neurological damage.
(NEVER ALTERNATE DOSAGES TO TAPER. IF YOU ARE SENSITIVE, THIS IS SURE TO SET OFF WITHDRAWAL SYMPTOMS.)
If you are a person who is sensitive to fluctuations in your dosage, you may be suffering quite a bit, and for these people, even if the original dosage is reinstated at this point, withdrawal symptoms may continue to be severe.
To save wear and tear on your nervous system, we recommend an initial drop of 10% and staying at that level for a month to see if withdrawal symptoms develop. If they do, you may wish to reinstate and make smaller decreases at intervals of about a month. If you are sensitive, this can protect you from a great deal of pain and discomfort.
If are not sensitive to a 10% drop, by listening to your body, you may be able to make 10% drops more often than every month.
In this way, the 10% method protects everyone and you have the option of tapering faster if you can tolerate it.
From the Icarus Project Mind UK Document
If you find you have to withdraw very slowly, it can be difficult to make small enough reductions in your dose, especially if your drug comes in capsule form. Sometimes it’s possible to break open the capsule and remove some of the content to lower the dose. You should always take care doing this, though, as the contents (for instance, fluoxetine) are sometimes irritating to the skin or the eyes. A pharmacist should be able to tell you if it’s safe to do so.
Some drugs are obtainable in liquid form, which can be diluted to make small reductions in dosage. It may be worth asking whether you can change to one of these. You would then need to be very sure what the concentration of the liquid is, and how much water to add to achieve the dose you wish. You may want to ask a pharmacist to help you with this….
Allow enough time for your body to readjust to the lower dosage at each stage. You could start by reducing the dose by 10 percent, and see how you feel. If you get withdrawal effects, wait for these to settle before you try the next reduction. Then reduce it by another 10 percent of the original dose. As the dose gets smaller, you may find this rate more difficult to cope with, and reducing by 10 percent of the reduced dose may be a better idea. If you started with 400mg of your drug, for example, you could first reduce the dose by 10 percent (40mg), to 360mg. The next 40mg reduction would take you down to 320mg, then 280mg, 240mg, and so on. If you got to 200mg and then found that a further drop of 40mg drop was too difficult, you could reduce by 10 percent of 200mg (20mg), and go down to 180mg, and so on. At each stage, if you find the reduction too difficult to cope with, you can increase the dose slightly (not necessarily back to the previous dose) and stabilise on that before you continue.
Also see Dr.Peter Breggin's 10% taper method
Please note that the 10% reduction method we recommend is a 10% reduction on the already reduced dose.
- If you started at 10mg, the first reduction would be 10% of 10mg, or 1mg, for a reduced dose of 9mg.
- Your second reduction would be 10% of 9mg, or .9mg, for a reduced dose of 8.1mg.
- Your third reduction would be 10% of 8.1mg, or .81mg, for a reduced dose of 7.29mg.
And so on.
This ensures that your nervous system is eased down a gentle 10% slope at every step of the process. It’s important that drops become smaller, not larger, as you go. Once you find the rate at which you can comfortably taper, you don’t want to jolt your nervous system with a larger drop than it can handle.
Mathematics whizzes may recognize that the 10% reduction formula is a geometric progression approaching but never equaling zero. At a very small dosage, likely less than 1mg, when reductions no longer cause any withdrawal symptoms, you will want to simply stop.
You will need to use your own judgment about your jumping-off point. Some people have found that the final steps require reductions so tiny they cannot measure them, employing methods such as dipping a toothpick in a liquid solution to ease off in the final stages.
By AltoStrata
AltoStrata's Surviving Antidepressants Web Site
Why taper by 10% of my dosage?
We believe that, for a minority, the risk of severe withdrawal is so great, a very conservative approach to tapering to protect everyone is called for.
Many people seem to be able to taper off psychiatric medications in a couple of weeks or even cold-turkey with minor withdrawal symptoms perhaps for a month or so. Doctors therefore expect everyone can do this. However, it seems a minority suffer severe symptoms for much longer.It is unknown how large or small this minority is. You may very well be in it. You cannot know how your nervous system will respond to a decrease in medication until you try it.
Withdrawal symptoms represent neurological dysfunction. Severe symptoms can be distressing, debilitating, or even disabling. If you get prolonged withdrawal syndrome, there is no known treatment or cure. You will have to cope with it until it goes away.
Some guides will suggest a trial decrease of 25% to start. If you get withdrawal symptoms, it is recommended to reinstate the original full dosage and taper more slowly from there.
That is reasonable, except that it can take weeks to feel the full brunt of withdrawal symptoms from an initial drop. If you have already made two reductions from your original dosage, you will have reduced by about 50% — and your symptoms may indicate substantial neurological damage.
(NEVER ALTERNATE DOSAGES TO TAPER. IF YOU ARE SENSITIVE, THIS IS SURE TO SET OFF WITHDRAWAL SYMPTOMS.)
If you are a person who is sensitive to fluctuations in your dosage, you may be suffering quite a bit, and for these people, even if the original dosage is reinstated at this point, withdrawal symptoms may continue to be severe.
To save wear and tear on your nervous system, we recommend an initial drop of 10% and staying at that level for a month to see if withdrawal symptoms develop. If they do, you may wish to reinstate and make smaller decreases at intervals of about a month. If you are sensitive, this can protect you from a great deal of pain and discomfort.
If are not sensitive to a 10% drop, by listening to your body, you may be able to make 10% drops more often than every month.
In this way, the 10% method protects everyone and you have the option of tapering faster if you can tolerate it.
From the Icarus Project Mind UK Document
If you find you have to withdraw very slowly, it can be difficult to make small enough reductions in your dose, especially if your drug comes in capsule form. Sometimes it’s possible to break open the capsule and remove some of the content to lower the dose. You should always take care doing this, though, as the contents (for instance, fluoxetine) are sometimes irritating to the skin or the eyes. A pharmacist should be able to tell you if it’s safe to do so.
Some drugs are obtainable in liquid form, which can be diluted to make small reductions in dosage. It may be worth asking whether you can change to one of these. You would then need to be very sure what the concentration of the liquid is, and how much water to add to achieve the dose you wish. You may want to ask a pharmacist to help you with this….
Allow enough time for your body to readjust to the lower dosage at each stage. You could start by reducing the dose by 10 percent, and see how you feel. If you get withdrawal effects, wait for these to settle before you try the next reduction. Then reduce it by another 10 percent of the original dose. As the dose gets smaller, you may find this rate more difficult to cope with, and reducing by 10 percent of the reduced dose may be a better idea. If you started with 400mg of your drug, for example, you could first reduce the dose by 10 percent (40mg), to 360mg. The next 40mg reduction would take you down to 320mg, then 280mg, 240mg, and so on. If you got to 200mg and then found that a further drop of 40mg drop was too difficult, you could reduce by 10 percent of 200mg (20mg), and go down to 180mg, and so on. At each stage, if you find the reduction too difficult to cope with, you can increase the dose slightly (not necessarily back to the previous dose) and stabilise on that before you continue.
Also see Dr.Peter Breggin's 10% taper method
Please note that the 10% reduction method we recommend is a 10% reduction on the already reduced dose.
- If you started at 10mg, the first reduction would be 10% of 10mg, or 1mg, for a reduced dose of 9mg.
- Your second reduction would be 10% of 9mg, or .9mg, for a reduced dose of 8.1mg.
- Your third reduction would be 10% of 8.1mg, or .81mg, for a reduced dose of 7.29mg.
And so on.
This ensures that your nervous system is eased down a gentle 10% slope at every step of the process. It’s important that drops become smaller, not larger, as you go. Once you find the rate at which you can comfortably taper, you don’t want to jolt your nervous system with a larger drop than it can handle.
Mathematics whizzes may recognize that the 10% reduction formula is a geometric progression approaching but never equaling zero. At a very small dosage, likely less than 1mg, when reductions no longer cause any withdrawal symptoms, you will want to simply stop.
You will need to use your own judgment about your jumping-off point. Some people have found that the final steps require reductions so tiny they cannot measure them, employing methods such as dipping a toothpick in a liquid solution to ease off in the final stages.
Subscribe to:
Posts (Atom)